Pelvic organ dysfunctions are complex and difficult to treat. These conditions affect a substantial portion of the population, especially with increasing age. Current stimulation therapies (Interstim therapy, Medtronic) have found no resonance in gynecology, while the vast majority of patients 70-80% are women. Further factors such as unfavorable reimbursement scenario (cost for neuroprothesis!) and lack of trained professionals are likely to pose a deterrents hampering market growth. Fro technical point o view, all techniques of implantation within the pelvic cavity are difficult to be reproduced by most gynecologists, while all techniques of implantation outside the protection of the pelvic cavity expose patients for lead migration and breakage. In this context, the stimulation of the genital nerves – GNS therapy – or more precisely of the dorsal nerve of the penis/clitoris (DNP) emerges as a very attractive alternative to other neuromodulative therapies that might result in great outcomes for controlling urinary, fecal and sexual disorders (see: Possover M. Minimally Invasive Two-passage Electrical Genital Nerve Stimulation: A Human cadaver study of a technique. Journal of Minimally Invasive Gynecology 2023 Jun;30(6):480-485. Doi: 10.1016/j.mig.2023.02.024).
GNS is the first method of stimulating pelvic nerves that does not require an operative test phase.
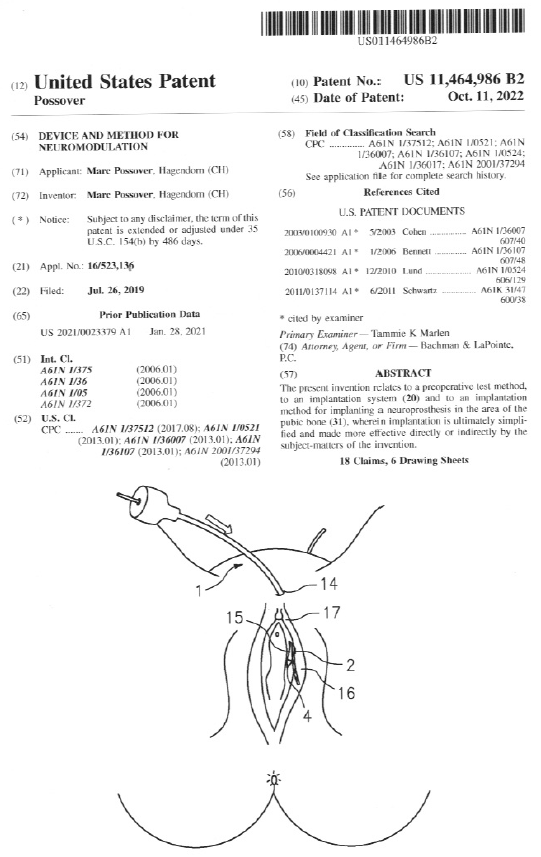
In neuromodulative therapies for pelvic organs dysfunctions, a temporary lead-electrode is traditionally placed surgically under general anesthesia to the nerves, in order to test the effectiveness of electrical stimulation on the symptoms. This test phase allows clinicians to judge how much a patient will benefit or not from a permanent neuroprothesis. In contrast to all current techniques , the GNS is the only one which does not require any surgical test-phase: Because part of the DGN lies superficially to the skin outside the pelvis, this nerve can be stimulated using surface adhesive electrodes attached to the overlying skin close to the vulva or the penis (Fig 1). Stimulation is simply achieved using a battery powered hand-held stimulator.
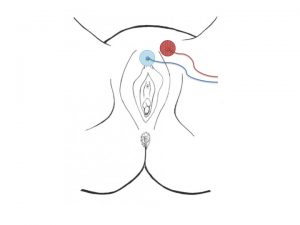
Fig. 1: placement of surface skin electrodes for DNP-stimulation
The effect of the stimulation can be tested by the patient in their daily, home and professional environment, or at the practice under urodynamic testing, or if required other electrophysiological testing.
The GNS-therapy is a procedure for implantation a permanent lead-electrode reproducible by every gynecologist trained in TVT procedure – one of the most frequent performed procedure in gynecology to treat stress urinay incontinence in women.
Studies using stimulation of the DGN have been performed more than three decades; the main issue still remains, the way of stimulation the nerve on long time. Stimulation using surface skin electrodes is limited for permanent stimulation, due to intolerance to required high stimulation amplitude. Surface electrodes have additional limitations such as difficulties in proper daily placement and issues related to hygiene as well as a lack of acceptance in some patients. Implanted electrodes are definitively more suitable. However, implanted electrodes in the penis or near the clitoris, must endure the mechanical stress of penile erections and external pressure, carrying the risk of the cable/electrode breaking or being and dislocated.
Thus the challenge was to develop an implantation technique that is minimally invasive, which allows :
– the implantation lead electrode in direct contact to the dorsal genital nerve outside the pelvis
– the implantation of the pacemaker within the protection of the pelvis (an implantation of the generator at the genital level is impossible!),
– the protection of electrode’s cable on its path to the pacemaker from external trauma (risk of cable rupture when it passes under the skin).
The GNS procedure offer all these advantages: lead implantation is obtained very easy by a vaginal retropubic approach using the „Curve Applicator, NeuroGyn AG, the cable is protected by the pubic bone while the generator is implanted through a suprapubic mini-laparotomy behind the pubic bone.